
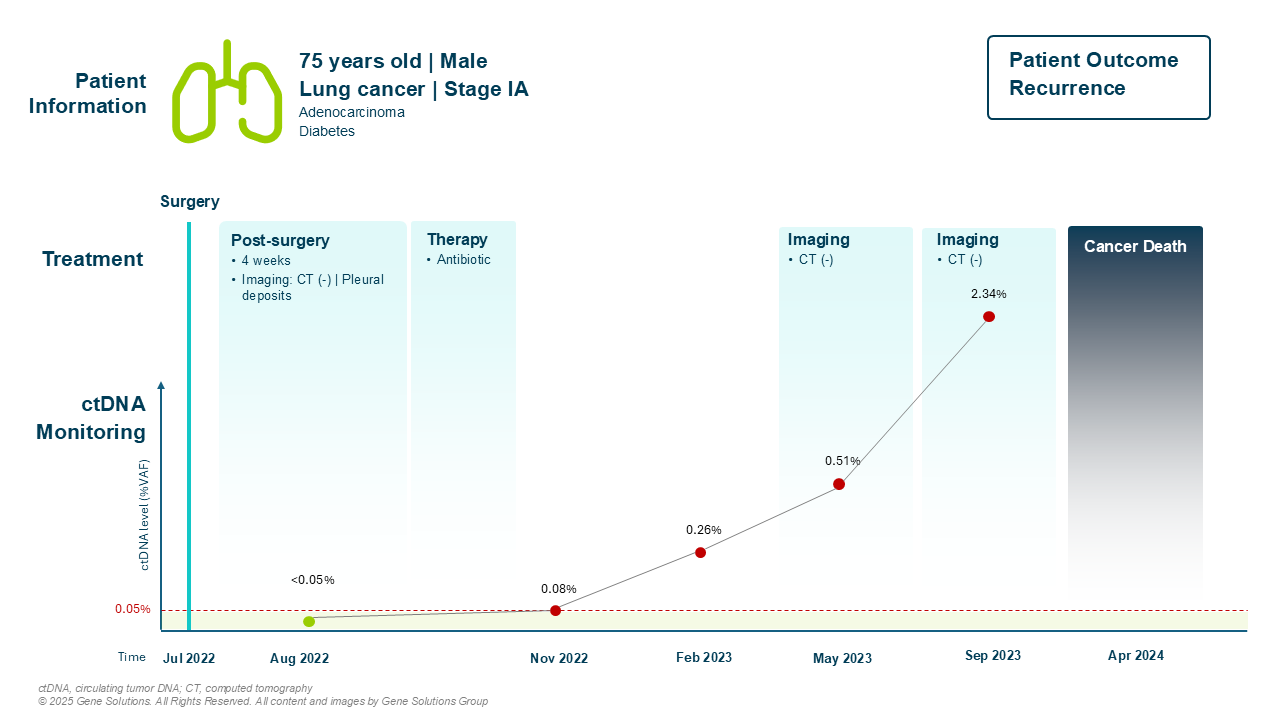
The patient was diagnosed with stage IA lung adenocarcinoma in July 2022. His tumor was small, resectable, and he underwent surgery without complications. The clinical outlook was optimistic — localized disease, and no evidence of lymph node involvement.
His physician took him in routine surveillance, including standard chest CT scans and circulating tumor DNA (ctDNA) testing. At landmark post-surgery, both imaging and ctDNA were negative. The early signs pointed toward recovery.
Four Months Later: First Signs from ctDNA
In November 2022, a surveillance CT scan showed mild pleural changes, which were attributed to post-surgical inflammation. Patient was placed on antibiotics, and clinically, there was no cause for concern.
But beneath the surface, something had changed. His ctDNA test came back positive, with a variant allele frequency (VAF) of 0.08%. While subtle, this result signaled minimal residual disease (MRD) — an early warning of potential recurrence. At that point, the imaging remained unremarkable. No therapy was initiated.
A Molecular Progression Without Radiographic Evidence
Over the next year, the patient’s ctDNA trajectory painted a concerning picture:
- February 2023: ctDNA VAF increased to 0.26%
- May 2023: rose again to 0.51%
- September 2023: peaked at 2.34%
All the while, chest CT scans continued to show no recurrence, and he remained asymptomatic. The molecular signal grew louder.
Final Outcome: The Recurrence Becomes Clinical
When ctDNA levels surged, a deeper analysis was performed. Genomic profiling revealed:
- EGFR exon 19 deletion – A targetable driver mutation with known sensitivity to EGFR inhibitors (1)
- ZFHX3 M307I and PTPRT P497H
These mutations provided important therapeutic insights — but by the time they were uncovered, the window for meaningful intervention had closed.
In January 2024, 14 months after the first positive ctDNA result, the patient passed away due to metastatic lung cancer. Despite consistently negative imaging, the molecular evidence had been present — and progressing — for over a year.
This case illustrates a sobering, yet powerful lesson: ctDNA monitoring can detect recurrence earlier than imaging in early-stage lung cancer. Had ctDNA results prompted earlier clinical action, the patient might have been eligible for targeted therapy based on his EGFR mutation — potentially altering the course of his disease.
Reference
- Herbst, R.S. et al. (2023) ‘Adjuvant Osimertinib for Resected EGFR-Mutated Stage IB-IIIA Non–Small-Cell lung cancer: Updated results from the Phase III Randomized ADAURA Trial,’ Journal of Clinical Oncology, 41(10), pp. 1830–1840. https://doi.org/10.1200/jco.22.02186.